
TL;DR:
- Having more healthcare providers involved does not automatically lead to better patient care.
- Structured coordination, shared decision-making, and integrated planning are essential for positive outcomes, especially in complex cases.
More healthcare providers involved in your care does not automatically mean better care. That assumption is one of the most persistent misconceptions in modern medicine, and the evidence tells a different story. The role of multidisciplinary healthcare, formally known as the multidisciplinary team (MDT) model, is not simply about assembling a group of specialists. It is about structured coordination, shared decision-making, and integrated care planning that genuinely changes outcomes for patients managing complex or chronic conditions. This article breaks down what that looks like in practice, what the data shows, and where the model is headed.
Key Takeaways
| Point | Details |
|---|---|
| MDT is more than adding specialists | Structured coordination and communication matter more than team size alone. |
| Evidence shows measurable gains | MDT models reduce readmissions, lower medication errors, and improve patient satisfaction. |
| Chronic and complex cases benefit most | Patients with multiple conditions see the greatest improvement under coordinated MDT care. |
| Implementation challenges are real | Leadership, training, and standardized processes determine whether MDT models succeed. |
| Shared decision-making is central | Involving patients in their own care plans improves treatment adherence and outcomes. |
The role of multidisciplinary healthcare defined
The term "multidisciplinary healthcare" is used frequently, but it is often confused with two related concepts: interdisciplinary care and integrated care. Understanding the distinction matters, especially if you are designing or evaluating a care model.
In a multidisciplinary team, each specialist assesses the patient independently and contributes their findings to a shared care plan. A physician, a pharmacist, a social worker, and a physical therapist may all be involved, but they typically work in parallel rather than together in real time. In an interdisciplinary model, those same professionals collaborate directly, often in joint case conferences, to create a unified plan where roles overlap and decisions are made collectively. Differentiating these models affects how governance and performance are measured.
The professionals most commonly involved in MDT-based care include:
- Primary care physicians, who serve as the central point of coordination
- Specialists such as cardiologists, pulmonologists, and endocrinologists
- Pharmacists, who manage medication reconciliation and polypharmacy risks
- Social workers and case managers, who address social determinants of health
- Nurses and care coordinators, who track adherence and flag early warning signs
- Mental health professionals, who address the psychological dimensions of chronic illness
What makes the MDT model effective is not the presence of these roles in isolation. It is how they coordinate. Shared care plans, defined communication pathways, and regular case reviews are what translate multiple perspectives into better patient outcomes. Without that structure, you simply have more consultations, not better care.
What the evidence says about MDT outcomes

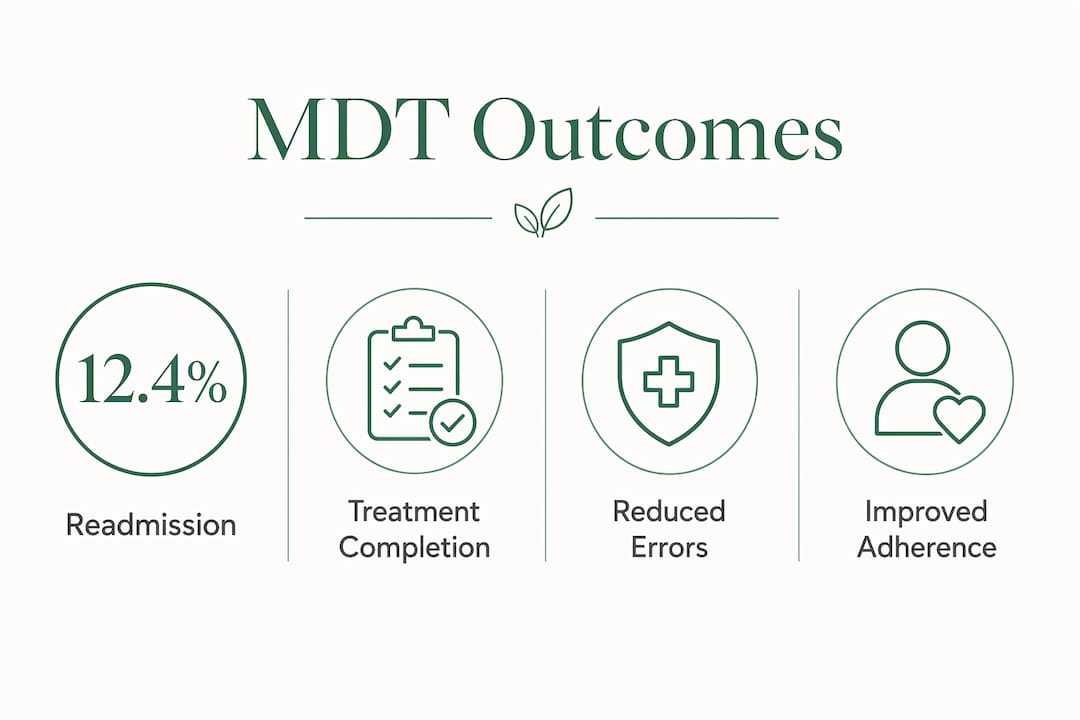
The clinical data supporting the MDT approach is both consistent and compelling. One of the most cited findings comes from a study of 348 adults with three or more comorbidities. The group managed under an MDT model saw 30-day readmissions drop to 12.4%, length of stay cut from 8.9 to 6.2 days, medication errors reduced by 56%, and care-plan compliance increase by 43%, alongside measurable gains in patient satisfaction.
Those numbers are not anomalies. In oncology, lung cancer patients in MDT programs showed a treatment completion rate of 86.09% compared to 68.57% in standard care, and median overall survival improved from 28.64 months to 45.21 months. MDT management also reduced unplanned treatment changes and kept patients on their prescribed pathways longer.
| Outcome Metric | Standard Care | MDT Model |
|---|---|---|
| 30-day readmission rate | Baseline | 12.4% |
| Length of hospital stay | 8.9 days | 6.2 days |
| Medication error rate | Baseline | Reduced by 56% |
| Care-plan compliance | Baseline | Increased by 43% |
| Lung cancer treatment completion | 68.57% | 86.09% |
| Median overall survival (lung cancer) | 28.64 months | 45.21 months |
For patients with multimorbidity, meaning those managing several chronic conditions at once, comprehensive geriatric assessments embedded within interdisciplinary care programs have been shown to reduce hospitalizations and emergency visits by identifying patient needs across multiple domains before a crisis occurs.
Pro Tip: When reviewing your organization's MDT outcomes, track both clinical metrics such as readmission rates and operational metrics like medication error frequency and care-plan adherence. Measuring only case discussion frequency gives an incomplete picture of how well your team is actually functioning.
The advantages of multidisciplinary care become most visible in patients whose needs cut across several disciplines at once. Coordinated MDT perspectives outperform simply adding more specialists because structured coordination addresses medical, psychological, pharmacological, and socioeconomic needs simultaneously.
What makes MDT models work and what gets in the way
Understanding why some multidisciplinary teams deliver strong results while others struggle starts with recognizing that the structure of care matters as much as the personnel involved.
The foundations of effective MDT implementation include standardized care plans that give every team member a shared reference point, defined communication protocols that prevent information from falling between roles, and regular case review meetings where findings are discussed rather than siloed. Effective MDT implementation also requires quality assessment practices, leadership commitment, and dedicated communication training. These are not optional additions. They are the mechanisms that turn a group of specialists into a functioning care team.
"Simply increasing team size does not guarantee better care. Identifying the key ingredients, including leadership, shared values, and effective communication, is what determines success in team-based care models." This finding from implementation science research in rheumatology applies equally across specialties.
The barriers to successful adoption are worth naming directly. Resource constraints remain a significant obstacle, particularly in smaller or community-based practices where staffing multidisciplinary teams is financially and logistically difficult. Information system fragmentation prevents seamless data sharing between providers. And cultural resistance within clinical teams, where professionals trained in independent practice may be reluctant to adjust their workflows, can undermine even well-designed programs.
There is also a common misconception worth addressing: that an MDT is simply a collection of consults. It is not. A consultation model places the burden of synthesis on one physician. An MDT distributes that synthesis across the team through structured processes. The difference in patient experience and clinical outcome is measurable. Learning more about what integrated healthcare means can help clarify this distinction for both clinicians and patients navigating complex care needs.
Practical applications and where MDT care is heading
For clinicians and policymakers looking to apply or scale multidisciplinary care models, several frameworks and strategies have proven reliable in practice.
-
Use an established framework as your starting point. The JA-CHRODIS multimorbidity model organizes multidisciplinary care around five areas: MDT delivery, individualized care plans, shared decision-making, information system integration, and community resource linkage. This framework directly addresses the fragmentation that undermines most standard care models.
-
Prioritize shared decision-making from the start. Involving patients in treatment decisions by incorporating their goals, values, and concerns improves both the patient experience and the effectiveness of care plans. Shared decision-making is not a courtesy. It is a clinical tool that increases adherence and reduces unplanned care changes.
-
Define roles before the team begins seeing patients. Role ambiguity is one of the most common sources of friction in MDT models. Each team member should know exactly what decisions fall within their scope, what information they are responsible for contributing, and how escalation works when clinical situations change.
-
Build measurement into your model from day one. Track readmission rates, medication reconciliation outcomes, and care-plan adherence as core metrics. Measuring only case discussion frequency tells you whether the team is meeting, not whether the team is working.
-
Plan for scalability with realistic resource expectations. Even well-designed MDT models face inconsistent delivery when resource limitations and quality measurement gaps are not addressed. Sustainability requires ongoing leadership support and a realistic assessment of staffing and infrastructure costs.
Pro Tip: If you are building a multidisciplinary team for chronic condition management, start with a small, well-trained core team before expanding. A focused group with clear communication protocols will consistently outperform a larger group without them.
My perspective on what MDT care actually requires
I have spent enough time examining how multidisciplinary teams function in real clinical environments to say this clearly: the biggest risk in adopting the MDT model is treating it as a staffing solution rather than a systems change.
I have seen practices assemble impressive teams on paper, physicians, pharmacists, social workers, care managers, and still deliver fragmented care because no one defined how information would flow between those roles. The team existed, but the coordination did not.
What actually works is a combination of deliberate process design, honest leadership, and a culture where clinical professionals feel accountable not just for their own discipline but for the patient's overall trajectory. That cultural shift is harder than hiring and slower than any policy change. But it is the variable that determines whether your MDT model delivers results like the ones the data shows, or simply generates more meetings.
The future I find most promising is the integration of social and community care into MDT models. Older patients managing multiple chronic conditions are not just managing disease. They are managing transportation, food access, housing stability, and social isolation. Teams that incorporate social workers and community health workers alongside medical specialists address a fuller picture of patient health. That is where the model is most needed and, honestly, most underutilized.
— Krunal
How Gardenstatemedicalgroup supports multidisciplinary care
At Gardenstatemedicalgroup, the multidisciplinary approach is built into the practice's structure, not bolted on as an afterthought. With locations in North Bergen and Secaucus, New Jersey, the group integrates primary care services, cardiopulmonary specialty care, radiology, and targeted health programs for conditions like diabetes, lung health, and bone health under a coordinated care model.
For patients managing chronic conditions, Gardenstatemedicalgroup's chronic care management program brings together the team-based coordination this article describes. Physicians, care coordinators, and specialists work from shared care plans with defined communication pathways, giving patients the structured support that leads to better adherence and fewer unplanned visits. If you want to experience what genuine coordinated care looks like in practice, Gardenstatemedicalgroup is a strong place to start.
FAQ
What is multidisciplinary care?
Multidisciplinary care is a model in which professionals from different specialties each assess a patient independently and contribute to a shared care plan. It differs from interdisciplinary care, where team members collaborate directly to build a unified, jointly developed plan.
Why choose multidisciplinary healthcare for chronic conditions?
Patients with multiple chronic conditions have needs that span several clinical domains at once. Coordinated MDT care addresses medical, pharmacological, psychological, and social needs together, which reduces hospitalizations and improves treatment adherence compared to siloed consultations.
What are the main advantages of multidisciplinary healthcare?
The core advantages include reduced hospital readmissions, fewer medication errors, higher care-plan adherence, and improved patient satisfaction. In oncology, MDT models have also been linked to significantly better survival outcomes.
What makes a multidisciplinary team effective?
Effective MDT models depend on standardized care plans, clear role definitions, structured communication protocols, and leadership commitment. Adding more clinicians without those elements does not reliably improve patient outcomes.
How does shared decision-making fit into multidisciplinary care?
Shared decision-making involves incorporating the patient's goals, values, and concerns directly into treatment planning. Within an MDT model, it improves adherence and ensures that the care plan reflects what the patient actually needs and can sustain over time.